How Soon Did Your Doctor Let You Lift Weights Again After Acl and Meniscus Surgery
What is a Meniscus?
The Medial and Lateral meniscal cartilages are gasket similar cushions in the knee. Positioned between the femur and tibia, they distribute the weight transferred from the larger femur in a higher place to the smaller tibia below. The Menisci likewise aid with the stability of the knee articulation. Good for you Menisci convert the relatively flat tibial surface into a more stable shallow socket
Why Practice They Tear?
Meniscal tears tin occur in any age group. In younger people, the meniscus is a adequately tough and rubbery structure. Tears in the meniscus ordinarily occur equally a result of a forceful twisting injury or with hyperflexion of the knee. In younger age groups, meniscal tears are more than probable to exist acquired by a sports injury. In more mature individuals, it can occur with squatting down, twisting or a fall. In older individuals, the meniscus can be weaker and easier to tear. Sometimes meniscal tears can occur equally a upshot of a minor injury, even from the up and down motion of uncomplicated squatting. Degenerative tears of the meniscus can also be seen as a part of osteoarthritis of the knee, gout and other arthritic conditions.
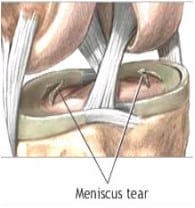
In many cases, human knee pain is the almost common complaint and the patient cannot retrieve one articulate associated injury that leads to the meniscus tear. The pain may be felt along the joint line where the meniscus is located. Sometimes the symptoms are much more than vague and occasionally they involve the whole articulatio genus. If the torn portion of the meniscus is big enough, locking may occur. Locking merely refers to the inability to fully straighten the knee or loss of the ability to move the knee. Locking occurs when a piece of torn cartilage, or meniscus, is stuck between the bones (see the picture above). In other words, the meniscus is caught in the swivel mechanism of the knee joint. Once stuck, it volition not permit the knee straighten out or move completely. (To see Dr. Reznik'due south video, "The Locking Knee", get to Youtube.com/DrAReznik.)
Left lonely, over time the locking and/or abiding rubbing of the torn meniscus on the articular cartilage will crusade damage or degeneration of the knee joint. As a upshot, the genu may likewise become swollen, stiff and tight.
Treatment: Meniscal Repair
One time a meniscus is torn, it won't heal on its own. The tear can be treated safely with an Arthroscopic procedure that Dr. Reznik performs equally an outpatient. It is often done under a light coldhearted with a local injection for post operative comfort. When the tear is repaired, Dr Reznik uses the arthroscope to place tiny sutures or stitches to fix the tear. Of the tears below the ones nearest the outer border are more often repaired, depending on the overall status of the cartilage. That is where the blood supply is all-time and the cartilage has the best chance of healing (the first, second and fourth images below). Radial tears (image viii below) can be repaired on rare occasions.

Meniscal Recovery Plan
Diet: You may resume a regular diet when yous return home. Start with tea or broth and advance slowly with crackers or toast, then a sandwich. If you become nauseated, return to clear liquids.
Pain Control: Accept pain medication as prescribed past Dr. Reznik. Please telephone call our office with whatever questions regarding your medication. Ice as needed (never place water ice direct on pare) and drag leg above heart level using 2-3 pillows. This will also subtract swelling.
Finish smoking: Smoking slows the healing process by interfering with the making of new DNA. Smoking also increases the risk of infection and pneumonia after surgery past slowing your body'due south white claret cells.
Deep Breathing: Exist sure to regularly accept a deep breath and blow it out. This helps to clear the lungs after anesthesia.
Knee Immobilizer: Meniscal Repair patients are to wear the genu immobilizer full time for the first iii weeks to protect the repair for the first phase of healing. This includes while you are sleeping. It is to be removed just for physical therapy directed exercises and showers.
Annotation: Patients should not flex the knee past 90 degrees for the starting time 3 weeks even if you therapist says information technology is okay. After three weeks, you volition change from the immobilizer to a articulatio genus hinged brace. This is unremarkably done past the physical therapist; if you lot or your therapist is unsure about what to use or when to change your brace call Dr. Reznik's function. Nether guidance, you can then start bending the knee from 90 degrees to a maximum of 120 degrees. When start switching to the knee hinge brace, you may need to use two crutches again for a brusk time to help with remainder if needed.
Crutches: Patients are to use two crutches for the first week, putting light weight on the operative leg with each step with the immobilizer on. Remember to put the involved foot flat on the ground. Almost patients can be fully weight bearing past the end of the offset week while continuing to wear the immobilizer. After the showtime week, y'all may then increase weight every bit tolerated and accelerate to one crutch for a few days and then a pikestaff if needed. Meniscus (cartilage) Repair patients cannot do twisting, pivoting, squatting, deep knee bends or impact activities for iv months. It is vital that meniscus repair patients practice not squat for at least iv months after the repair.
Return to Work: People with light work (like desk-bound or figurer work with no squatting, lifting or kneeling) can return to work within a calendar week to ten twenty-four hours with the brace on. The exception is for people who may take long commutes. Past staying still with the leg downwards for long periods, increases the risk of a BLOOD CLOT in the leg. Patients with agile office work or very lite labor with variable tasks can sometimes become back to work at two or three weeks, depending on lifting requirements and if their employer will make accommodations for light duty. Heavy work, (lifting or unprotected heights) cannot usually render before six weeks. Most will need to be cleared by their physical therapist. The heaviest of labor, working in unprotected heights would naturally take longer. Driving: Right human knee patients and left genu patients with a standard transmission car cannot drive until out of the knee immobilizer, off all pain meds and tin can fully weight bear without pain. Left genu surgery patients tin can drive after iii weeks if they have no pain and you are off hurting all hurting medications comfortable walking without crutches.
Claret Clots: Those at higher risk of blood clots include those patients who take sedentary life styles, long car or train commutes, take a history of prior cancer, women on nascence control pills, may be overweight or males over the age of 40. These patients should be taking an at least a baby aspirin per day (unless allergic or sensitive). Doing the exercises (talocrural joint pumps below), using aspirin and at times compressive stockings volition also reduce the risk of blood clots. Patients who accept a history of clots in the past or three or more than of the above risk factors should ask if they should be on a blood thinner mail service op for at least six weeks.
Call the Physician If:
- You develop excessive, prolonged nausea or airsickness
- Fever above 101
- You lot develop any type of rash
- Y'all experience calf pain
Post-Operative Exercises: Start doing exercises while nonetheless in the recovery room. Dr. Reznik or your nurse will instruct y'all on what to do. At abode, while resting in bed afterwards surgery do the following every hr or with each set of TV commercials.
Ankle Pumps: Pump your ankle up and down for ane minute (like pressing on the gas pedal). This will increase circulation and reduce the gamble of developing a blood jell. If watching Idiot box, do this during every commercial.
Direct Leg Raise: Tighten your quads (muscle in the front end of your thigh) with the knee immobilizer on and enhance your leg eight to 12 inches off the bed. Do at to the lowest degree three times a day.
Add other exercises as your therapist gives them to you.
Knee bends/heel slides: With your heel on the bed, bend your knee joint while sliding your heel toward you. Start with bending 30-45 degrees and work toward xc degrees during the first week.
If you are in bed for extended periods, move your artillery regularly. Use light weights for upper arm exercises and keep muscle tone for using crutches.
Source: https://www.ct-ortho.com/patient-resources/patient-education/articles/torn-meniscus-repair-and-post-op-instructions/
0 Response to "How Soon Did Your Doctor Let You Lift Weights Again After Acl and Meniscus Surgery"
Post a Comment